We live in an age of digital scams. Not a day goes past when
we aren’t tempted by emails or other messages from nefarious individuals
attempting to extract money. Why should academic journals be any different?
A couple of decades ago, it was challenging to manage an
academic journal; snail mail, printing costs, office rental, advertisers etc.
The digital age and the open-access movement have made it such that anyone with
some decent IT skills can create an official looking scientific journal in their attic.
The opening of this study does a great job of summing up the
current state of play.
Thousands of academic
journals do not aspire to quality. They exist primarily to extract fees from
authors. These 'predatory' journals exhibit questionable marketing schemes,
follow lax or non-existent peer-review procedures and fail to provide
scientific rigour or transparency.
Crucial to the quality of an academic journal is its editors.
They should have a strong research background, been involved with peer review
and ultimately qualified for the job.
These researchers from Poland concocted a sting to see if a “dismally
inadequate” scientist would be invited to be an editor. They created the profile
of “Anna O. Szust.” (Oszust is the Polish
word for “a fraud.”)
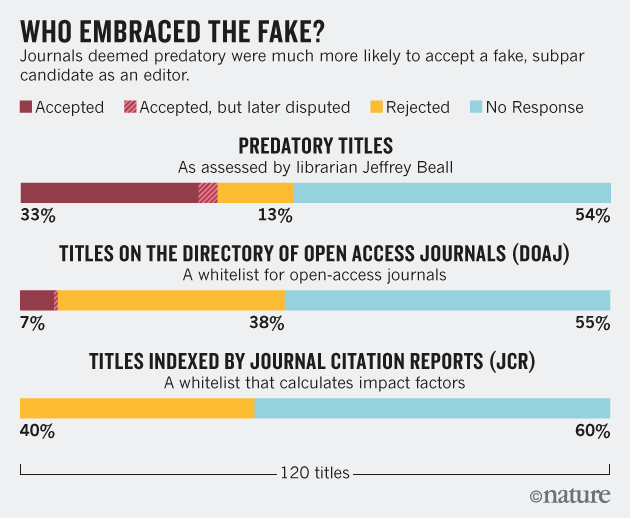
Her CV and application was sent to 360 journals. They were sent to one
of three directories; the JCR (journals
with an official impact factor), the DOAJ
(Director of Open Access Journals), and finally to a group thought to be predatory journals (from Beall’s list).
Results?
None of the JCR journals accepted the application. By comparison,
40 predatory and 8 DOAJ journals appointed her as editor. There were some hilarious
and sometimes disturbing responses from the journals. I strongly encourage people
to read
the original manuscript at this link
What should we take away from this?
- There are over 10,000 predatory journals on the planet that do not exist for the advancement of scientific knowledge. They are fraudulent and have been created to make money.
- Be VERY sceptical of papers published in predatory journals. They were likely accepted not on their merit & methodologic rigor but rather their ability to pay a fee.
- If you are a researcher looking to publish a study, do your homework. Ensure that the journals you engage are known to be reputable.
Covering:

